
Blood Pressure
Curiosity
As the saying goes, curiosity killed the cat. It may be the death of me also because there are so many things that arouse my curiosity. Take blood pressure for instance. My Doctor said, that for me (and 20% of the UK’s older population) blood pressure is too high (Fig 3). “you will have to take tablets for the rest of your life” he advised. As I am unhappy with taking any medicine long term,(see note 1) I have searched for another option. First I purchased a meter(Omorn 711) which I am told measures blood pressure. At least it measures the same thing as the doctor’s instrument, and gives similar results. But I reserve my opinion as to whether its only Blood Pressure that is being measured, for reasons I will explain later. My first observation is that the measurement is not consistent. Allowing the recommended two minutes between measurements I frequently observe variations between successive readings of 14% (16mmHg systolic, 8mmHg Diastolic) But this can also be the difference between an acceptable normal reading and an alleged hypertensive one (Medical term, for danger level). Doc explained they work on statistics. And more people with mainly hypertensive readings suffer heart attacks than those with mainly normal ones. So they prescribe life style changes and / or tablets which lower blood pressure (my tablets on average lower it by the same 14%). In point of fact the risk of stroke rises in a continuous reflection of blood pressure levels (Lancet 13/12/02) so it is questionable which level is to be considered hypertensive. For concerned people it is important to get this into perspective. Its all very well to be aware that “more people with mainly hypertensive readings suffer heart attacks than those with mainly normal ones” But how many more? And what is the risk of heart attack anyway? National statistics (see note 2) show that only 1.0% of the population die of unnatural causes and only 0.1% through having a stroke (see note 3). The latter represents a probability of 1 in a 1000. An insignificant risk. While it is reassuring that the greatest single risk we have to face, at least in the Western World, is comfortably low, it is understandable that the doctors should give the greatest single risk a lot of attention. A 1998 trial claimed 23 strokes in the treated group compared to 44 in the untreated group but overall deaths during the trial were similar in the two groups. The implication is that treatment (mainly Beta Blocker and Diuretic) makes death from other causes more likely. It is well documented that anxiety can affect the blood pressure (BP) measurement . And I have noted an immediate rise of 16% between successive readings when my thoughts wandered to a stressful situation (and a fall of 6% after a shot of rum, unfortunately not available on prescription). If one were to argue that ideally blood pressure should stay about the same, then the variation seen in a young persons blood pressure could indicate the sort of variation we could expect from mental pressures and anxiety alone. This is about 80mm Hg, about 50% of the reading in a hypertensive man. There is a supporting argument, for viewing anxiety independently from BP, from the observation of pulse rate and blood pressure, in that while BP readings can range over about 40% the pulse rate readings stay within 15%. But we know that with exercise it is the pulse rate that is increased, up to twice the normal rate(+100%), to increase the blood supply. So if the pulse rate is the preferred method of increasing blood pressure, and therefore blood flow, why is it not used also to support anxiety? Is it because in anxiety it is muscle tension that is being increased and not the blood pressure, but none the less affecting the blood pressure measurement? So it could be argued that the mental component is a significant part of the perceived problem. An experiment in which TV was banned for a few weeks on the basis that its emotionally disturbing and emotions effect the blood pressure readings had the dramatic effect of reducing the average mid-day and evening measurements by a significant amount. If that draconian treatment is thought to cost too much, It may well be that careful choice of program and self discipline would do the something similar. We might well ask then are we sure that the measurements we are taking are in fact the pressure of the blood in the system or is it possible that we are being misled by an established practice. Let us examine the procedure. The measurement is taken with a sphygmomanometer. The instrument inflates a cuff around the arm until it stops the blood flow and it is the air pressure in the cuff at this point, that is taken as equivalent to the systolic blood pressure measurement. This assumes that there is no other component resisting the air pressure, only the force behind the blood, but the cuff encircles the whole forearm so it is the arm that must be considered as the blood vessel. The artery is surrounded by bone one side, and the controlled flexibility of the muscles on two sides. These components can not be dismissed as not having some effect resisting cuff pressure.. It could be that it is the flexibility of the arteries and surrounding muscles that is responding to the emotions and is effecting our measurements. Let us try to imagine what the effect of controlled flexibility would have on blood pressure readings taken with a sphygmomanometer. If the blood vessels were inflexible, say they were made of iron, and were only using reasonable pressure, we would not be able to obtain a reading at all because the iron pipe would resist any reasonable pressure and could not be pressed flat to stop the blood flow. A flexible pipe would still resist the cuff pressure depending on its level of inflexibility so the reading on the sphygmomanometer when the blood flow stopped would not represent blood pressure alone but the sum of the pressure needed to overcome the inflexibility of the artery and other muscles, plus the pressure needed to stop the blood flow. But if the inflexibility is controlled in part by the emotions then we might expect the sort of reading that we get in practice. The difference between the reading taken when we are calm and the reading taken when we are anxious would not then be due to increased blood pressure alone but in part due to the emotion affecting the flexibility of the blood vessel which is acting as an interface. We now have two contrary theories. The traditional one that the sphygmomanometer is measuring blood pressure and if the measurement gets too high you are in danger of bursting a blood vessel causing a stroke. And the theory outlined above that the sphygmomanometer measures two separate things and adds them together. Only one of which is the critical blood pressure. The point is that the traditional theory can be very stressful producing a vicious circle that increases the anxiety related blood pressure measurement still further. But if the second theory is correct and stress can be separated out from BP then we would have been worrying unnecessarily. We have built a model of the circulatory system (See Fig 1)
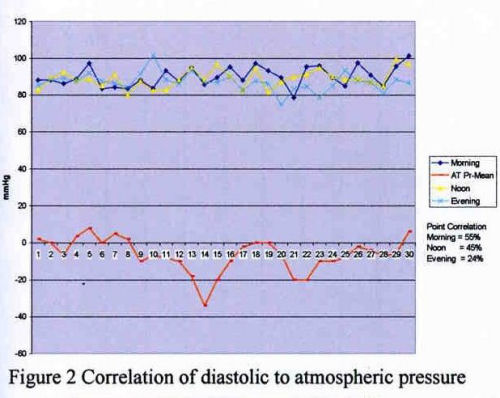
from a pump and polythene tube to see if the effect can be simulated. The surprising result is that the pressure measured as that to stop the flow is actually the pressure required to divert the flow into other loops of the circulatory system. It is not possible to stop the flow, in the model, with any pressure within the range of the BP meter even when the pump flow is minimum. What is being measured is the resistance to flow presented by the rest of the system at the point of measurement. It is a measurement related to blood pressure but not directly as the conventional explanation of the procedure suggests. Our confidence level in the resulting statistics may not be justified. It might be argued that it does not matter if BP readings are even related to blood pressure the statistics would remain valid. I agree that they would but the treatment reduces only the Blood Pressure, while the extra mmHg may be due to muscle tension. The effect would be seen as the same and the treatment would be assumed to be working. Where as in fact you would be reducing blood pressure to below that was biologically required, and not treating the muscle tension that was incorrect, compounding the biological error, and at the same time masking it. Not, I would have thought, in the best interests of medical science, nor the patient and it would do nothing to correct the statistics. The chance of a stroke would remain the same for this group provided the distorted blood pressure did no harm. Another possible mechanism which could raise BP is due to Cholesterol an essential component of blood which if present in too high quantities can be laid down on the inner walls of blood vessels making them narrow and putting up BP. The circulation system is composed of many loops each or any of which could develop localised deposits giving localised raised BP, otherwise one or two examples of low readings each month could be enough to indicate that the danger was remote. But a low, or high, reading in the arm loop does not imply the same pressure exists in every loop . Fortunately the risk can be avoided by eating less animal fats and reading the small print on packaged food to minimise sodium intake. But apart from the mental state and cholesterol there is another effect that seems to have some correlation with the readings but could be independent of any other possible cause. The Doctors measuring device is a sphygmomanometer which measures the pressure in the cuff above atmospheric pressure in units of mm of mercury. If the atmospheric pressure changes the sphygmomanometer reading changes by the same amount. So for the same blood pressure (and mental state) the sphygmomanometer will only give the same reading if the barometric pressure has not changed. But atmospheric pressure can vary from day to day as much as 6%. It might be thought that the blood pressure is also subject to atmosphere but, unlike the sphygmomanometer the Circulatory system is a closed loop. It is controlled by the autonomous nervous system so could be totally independent of atmospheric pressure. In fact comparisons of atmospheric pressure with my blood pressure show an average positive correlation6 of about 33% (See Fig 2) But surprisingly, an overcompensation. This is only an indication as the sample was limited to two, I hope to find a number of sufferers with there own blood pressure meters to conduct a more creditable test.
The level of fitness can also modify readings as does keeping ones weight to the recommended levels. Regular exercise can reduce the readings. An hours walk has been personally documented to reduce readings by 15% for two or three hours with an additional progressive effect (because, with greater use, the blood vessels feeding the muscles grow bigger. This lowers the resistance to blood flow and therefore the pressure required). The advice of BUPA is for 12 sessions a month of exercise vigorous enough for it to become somewhat difficult to find time for speaking between breaths. But I am curios why all this hard work is advised if a gentile exercise like walking can do the same thing. With gentile exercise you don't raise the pulse rate or the blood pressure abnormally. I would have thought that it was high blood pressure with its increased risk of stroke that we want to avoid!. The assertion that a sphygmomanometer measures Blood Pressure when its measurement is apparently the sum of three or more different varying parameters (BP, Barometric Pressure, and Mental state) is like trying to tell the time from an accelerometer! There is a time factor where it is true (Just as there is a blood pressure factor in a sphygmomanometer reading) but its distorted by other parameters. And any serious value, for gauging the need for Blood Pressure medication, must be more due to the measure of the judgement and experience of the operator than to the specific reading. We can propose a better measuring device. One which can separate out the parameters. An Improvement may be a device which was compensated for atmospheric pressure, which could be done by the addition of a barometer to a sphygmomanometer. This would remove one of the parameters but if the body does overcompensate we might find we end up with a more accurate but even more confusing reading of blood pressure than we have now. If in addition automatic compensation for the mental state was possible by measuring muscle tension, we might take some of the uncertainty away from the diagnosis. This does seem practical.. We are not much further forward except for the appreciation of the limitations of the present instruments which indicates we should not be panicked by Hypertension. Meanwhile we can look forward to developments that will measure our blood pressure with increased accuracy though that will mean we will have to start all over again with the statistics. By taking reasonable precautions and using a meter with understanding you may be able to avoid adding unnecessary anxiety to the doctors prophesy. The Author intends to persevere with this research and is looking to form a group of supporters in order to ensure that we can place a better and more accurate instrument in the hands of our experts. Note 1. I believe that the bodies design is incompletely known to our experts. What they are working on is a large collection of observations which they do their best to make sense of. But experts are not God and they can, with the best of intentions be misled. My attitude is to take medicine only as a temporary help. If you do not get better or if you then get worse, the medicine is worse than its cause and then experts are as likely to make matters worse as they are to make them better because we have obviously moved out of their area of expertise (and into the area of guinea pigs). Even if we, and they, like to believe something different! I guess that's the time to turn to God. Professor Beevers in a BMA publication on blood pressure seems to be saying "God knows" when he quotes a definition of hypertension as "that level of blood pressure where the treatment with antihypertensive drugs does more good than harm. One assumes then that the long term taking these drugs can have a harmful effect. Note 2. Social Trends HMSO 1998 7.24 (638,900 in 60M) Note 3. Health Encyclopaedia Royal Society of Medicine. Note 4. As a rule of thumb I would rate any risk greater than one in one hundred as insignificant and most unlikely to happen i.e. not worth the worry. Note 5. BMA Family Doctor Guide pp 13 refers to the blood flow as stopped when the sound, heard in the stethoscope, ceases. but the sound is absent before the cuff is inflated, and the flow is not stopped then. We can take a clue from Hydraulics where it is noted there are two modes of fluid flow, "smooth and quiet" and "turbulent and noisy". The operational mode depends on the pressure and diameter of the vessel, among other things. The conditions of normal blood flow in the arm equates to the quiet mode but restricting the vessel with the air pressure in the cuff may be presumed to instigate the noisy mode, because that is what the doctor listens for. But it seems to me a bit of a big jump to assume that when the noise stops it must be because the flow has stopped, indeed the model indicated otherwise. Note 6. There is a traditional correlation formulae using "Standard Deviation" (a measure of dispersion) which produces similar, not identical, results but it is designed for population statistics and not to compare waveforms in a point by point mode. It is not at all easy to visualise the rational. The Author prefers the following method. A measure of correlation might be obtained even when several variables are added to form a waveform by taking regularly spaced sample points from the summed waveform and comparing them for + or – slope to the same points on the suspected component waveform. This is based on the assumption that change of slope will not occur in all component waveforms at the same time. The scale of the components is ignored. Add the points in agreement and take them as a % of the measured points as a measure of correlation of change. If the points were purely random we could expect a result of 50% this represents no correlation. But measures of less than 50% are still correlation. The measure increases as it moves away from 50% Then correlation % = {X*100/X+Y} - 50 *2 Ignoring sign Where X = Number of points in agreement And Y = Number of points in disagreement This Formula has been developed to subtract the 50% that represents zero correlation express it as a % of the number of points. This gives a better agreement with human judgement. Neutral gradients c/f Non-neutral taken as differences. And neutral c/f neutral are counted as the same slope. Note 7. British medical Journal 1st November 1986
Curiosity - News Letter. March 03
Roy Miller's update on Blood Pressure investigation.
comment welcomed roy@themillersathome.co.uk Essential hypertension in my understanding, is the name given by Doctors to higher than normal Blood Pressure for which they can find no cause so far, and I share their curiosity. Perhaps the cause is elusive because it is not medical. My suggestion that it might be due to physical size will require testing but the theory is a bit more than a guess and I will explain my reasoning.
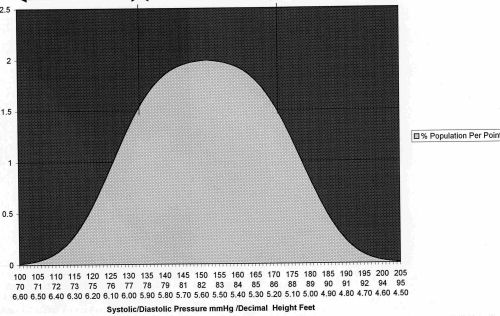
It is suggested that the profile of all blood pressure readings follows the same line as many other personal characteristics (i.e. Height, IQ etc) and forms what is known as the Normal Distribution represented above. This Graph arguably represents the percentage of the population (vertical axis) who's average diastolic BP is noted on the horizontal axis. The Graph suggests that 70% of the population have a diastolic BP between 63 - 110mm HG. But other characteristics of man such as Height and weight, which follow the same line, suggest to me a relationship. Is it possible that at least some "Essential Hypertension" is simply the result of a persons size? I can find no BP trial that takes account of a persons size but women are on average smaller than men and trials do reveal they have higher average BP. But why should a smaller person have a higher blood pressure? Well because pressure in simple terms is force divided by area (which is why a lady wearing stiletto heels exerts more Pressure on the floor than the same lady wearing trainers. Its the same force -the ladies weight - but applied over a smaller area, so the pressure is greater and potentially more damaging to the floor.) But in our case the "area" is proportional to the cross section of the blood vessel which might be thought to be smaller in a smaller person. Even a small trial which included the persons height would give a good indication. If other people with Blood Pressure problems would kindly send me their average blood pressure reading together with their height, I promise to publish the result when I have received 100 readings.(Email above). Roy Miller RMN FIdiagE (Sadly, Roy can't meet this commitment any more however, his study would be a good basis for a degree thesis. Do you know any science or medical students looking for an interesting idea?) Web Master